Hw Does Vietnamese Family Pick Out Healthcare Doctor in U.s
In many countries, family medicine or general practice has been established and developed over decades, with high percentages of medical students becoming family doctors (or general practitioners) after graduation.one–4 In Vietnam, customs or district health centres (CHCs) and district hospitals are the most important facilities at the primary care level. Yet, most CHCs do non accept a family medico; 30% of CHCs practice not even have a medical medico.4 The lack of resource and limited medical facilities (eg restricted medication prescription list and the unavailability of blood testing) results in low quality at the principal care level and is the main reason why patients bypass community and district levels and go directly to provincial hospitals, although most of their illnesses can be diagnosed and treated at a lower level.
In 2013, a national plan for family medicine evolution was established to better the quality of primary intendance (called Circular No sixteen). For the period 2016–twenty, the Ministry of Health approved the piloting of family medicine clinics in eight of 63 provinces/cities, expected to expand up to 80% of provinces/cities throughout the country by the year 2020.5 According to this policy and an updated Circular in 2019 (chosen Circular No 21, which replaced Circular No 16), family doctors can work in either a CHC, an out-patient department of a district hospital or a full-time or part-time private clinic. Each university medical heart has non only been a clinical practice site, but besides ane of the airplane pilot family medicine clinics in the national strategy (Figure 1).half-dozen,seven Currently, preparation family unit doctors and family medicine module(s) for undergraduate students take become mutual in well-nigh medical universities. So far, visits to family doctors in some pilot clinics have increased, just family medicine–based care is not mutual and recognised by the community.
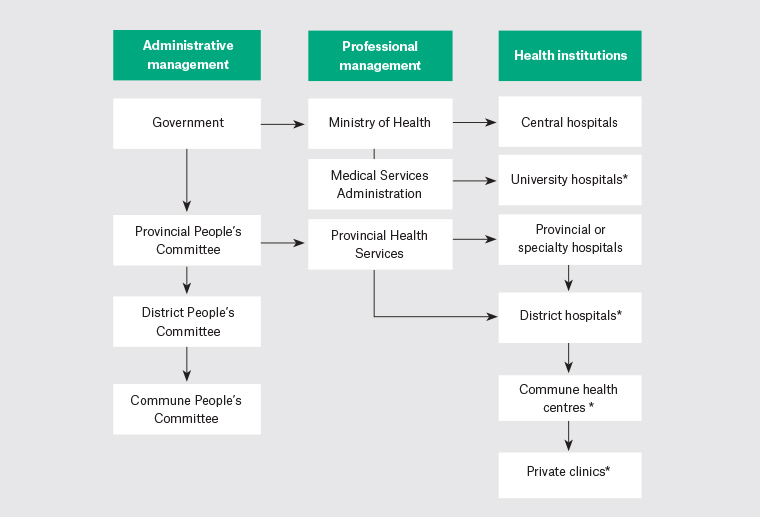
Figure 1. The Vietnamese healthcare arrangement
*The different institutions that contain pilot family medicine clinics (post-obit the Round No 21/2019/TT-BYT of the Ministry building of Health)
For many years, a main resource for CHCs and commune hospitals has come from upgraded doctors. An upgraded md is a physician who completes a four-twelvemonth additional training plan later on completing a three-year banana physician programme and has been clinically working for at to the lowest degree 12 months. The duration of the principal medical training program is six years. Family medicine has been taught mainly in the two-year postgraduate programs (called specialist level 1) since 2003 and in a 3-calendar month continuing medical educational program for licensed medical doctors since 2014. Since 2017–xviii, a two-week family medicine rotation has been integrated into the undergraduate six-twelvemonth and four-year medical programs. A previous study showed that the family unit medicine rotation had an bear upon on students' knowledge, attitude and skills towards family medicine.eight Nevertheless, the lower condition of family unit medicine in comparison to other specialties may atomic number 82 to low levels of involvement in this discipline by students and medical staff.
At nowadays, determining how to concenter medical students to piece of work in primary care is a common question in many countries.nine–12 Research in several countries has shown that interest in and career option toward family medicine or primary intendance depend on many factors: medical student aspiration for high status specialties, the representation of the profession, presence of training in this discipline in undergraduate programs likewise as training duration.thirteen–17 Senf et al reviewed 36 articles on family medicine specialty choice that were published betwixt 1993 and 2003. Students who believe chief care is important, have a rural background, have low(er) income expectations, have career intentions at entry to medical school and do not plan a enquiry career are more likely to cull family unit medicine. The time dedicated to family medicine in clinical years is related to higher numbers of students selecting family unit medicine. Kinesthesia role models take both positive and negative influences.eighteen
To these authors' knowledge, no study has been conducted into how students perceive family unit medicine and their potential career choice in the context of a new family unit medicine module introduced into undergraduate training and the national supportive entrada in developing countries such as Vietnam. The objective of this study was to explore how 6th-year medical students perceive family medicine after having completed an feel-based module on family medicine, and to explore which factors influence their selection for a career in family unit medicine.
Methods
Report design
This was a qualitative research study with in-depth interviews and focus group discussions. Thematic assay was used.xix–21
Participants
The study was carried out among sixth-year medical students who had completed the fifth-year family medicine rotation the first time information technology was offered at Tin can Tho University of Medicine and Chemist's, Vietnam. The sample included viii in-depth interviews (DIs) and iv focus group discussions (FGDs) with 36 students. A criterion sampling technique was used to recruit a heterogeneous group of medical students from different grade groups; students in i FGD all belonged to the aforementioned class. Participants were recruited with the help of course monitor students who identified students who showed interests in the inquiry topics and could requite rich data. The sample had an equal distribution in students' sexes and origins (rural/urban area). No participant refused to bring together the study. More DIs and FGDs had been planned in the outcome the information was not saturated, simply this proved unnecessary.22–24
Research team
The research squad consisted of experienced researchers in education, quality research, family medicine and community health. The facilitators of the FGDs and DIs were teachers in public wellness and family medicine.
Data drove
Information collection period
Data collection was carried out from Jan to March 2019. This period was the students' twelfth (concluding) semester. The students had completed a family unit medicine rotation in their tenth semester and other courses in near specialties and subspecialties after that. They were interviewed half-dozen months earlier they graduated to become medical doctors.
Data collection methods
A conceptual framework was built to explore the possible influencing factors on students' interests (Figure 2) on the basis of a literature review and the experience of the enquiry team. From that, a question guide for DIs and FGDs was developed. To ensure that the question guide was valid, a pilot written report was washed with a DI and an FGD with eight students in November 2018. After being piloted, the club and further exploration of dissimilar parts of the question guide were adjusted (Box ane).
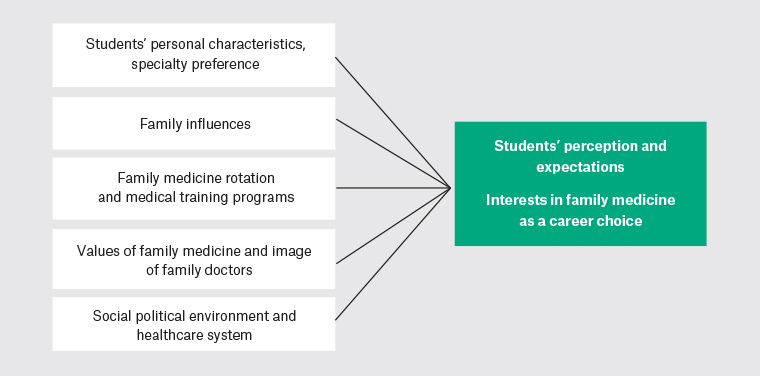
Figure 2. Conceptual framework of students' perceptions of and interests in family medicine and some possible influencing factors
| Box ane. Question guide for in-depth interviews and focus group discussions |
| 1. Cocky-introduction Tell me most yourself: Where are yous from (proper name of province, rural/urban area)? Which rotation are you lot now taking? ii. Perceptions towards family unit medicine You studied family medicine a yr agone. What exercise you understand about this discipline? (Describe in detail, in your ain words, the work or practice of family doctors, and their roles in the wellness system.) 3. Interests in family medicine, at a sure model/practice identify Considering there are three different models of family unit medicine (commune health centre, commune hospital, private clinic full fourth dimension/function time), delight tell me in detail virtually your interests in each model. Please explicate more virtually this. 4. Career choice in family unit medicine, and at a certain model/do identify How likely is information technology that you will choose family unit medicine for your career? Delight explicate more about this. v. Factors influencing your career option in family medicine Which factors are important for your pick of specialty? Please explicate in item. Example: Is the place where you'll alive of import? Other factors to exist considered: piece of work–life balance, income, academy, training programs, wellness policy, other? |
The DIs and FGDs took place in comfortable meeting rooms or offices in the academy simply outside the family unit medicine section. Both types of interviews lasted betwixt lx and 90 minutes. All DIs and FGDs were digitally recorded and transcribed verbatim to facilitate subsequent data analysis. The rules for FGDs were verbally introduced to participants to engage them and permit them to feel comfy in the discussions. 1 of the two interviewers facilitated the discussions or interviews while the other acted as an observer (to gain more than non-verbal data) and secretary (to accept field notes of the interview). Before the discussions, the first author – who was likewise a family medicine teacher – introduced the study objectives to the participants, but she was non present during the meetings.
Information assay
The authors used line-by-line coding of each case's interview responses, followed by a comparative thematic analysis of all cases. The researcher and the ii interviewers independently coded each interview, and all codes were entered manually into an Excel matrix. Next, the authors met as a team several times to discuss the codes and identify emergent themes until a concept map that represented the study's findings could be developed. The DIs/FGDs were conducted in Vietnamese and so analysed in the native language to completely understand what was meant in the appropriate context. Afterwards that, English translation of the main findings was performed to allow discussion with the non-Vietnamese co-authors.
The group of native linguistic communication–speaking analysers discussed any disagreements about emergent categories to make sure that the participants' points of view were captured. This process of cross-checking coding of the major categories provided 'thoroughness for interrogating the data' and helped while analysing the interview data.
Ethical issues
The enquiry protocol was approved past the Ideals Commission of Tin Tho University of Medicine and Pharmacy (HE20180012). The study participants were well informed about the study and gave their oral consent to being interviewed. Their anonymity was protected and guaranteed by the researchers. The participants had finished their clinical rotations in family unit medicine department, so their responses would not influence their study scores or examinations.
Results
Participants
There were 36 students participating in this study. Viii students were interviewed with DIs and 28 students participated in four FGDs (an average of seven students per FGD). Sex was every bit distributed in both DIs and FGDs.
Perceptions nigh the roles of family doctors and benefits of family medicine for healthcare
Nigh students were able to describe what they learnt about the roles of family doctors. They understood that family unit doctors were doctors who provided intendance that was continuing, comprehensive, preventive and family focused. Particularly, they appreciated that one of the important roles of family doctors was the management of common chronic diseases.
I think that family unit doctors take an reward that they see all members in the same family unit and follow upwardly them in a long term. In improver, family medicine tin be at community, district or central [provincial] levels. Family doctors can perform screening, first contact, often manage common diseases, chronic illnesses, long-term diseases, inherited diseases and screening for families. [Female person educatee (FS), DI-1]
All students recognised the benefits of family medicine equally 'reducing healthcare cost for both patients and the healthcare organisation, reducing hospital overload and mortality rate. Family unit doctors were able to aid many people, and so family medicine could amend the chapters of health staff also every bit improve patients' trust on wellness staff at lower levels of intendance' [FS, FGD-1].
Most students agreed that family doctors could piece of work at most levels of the healthcare system. They recognised that in that location is a big need for this kind of dr. at principal care level including CHCs, district hospitals, private clinics and even provincial hospitals.
Interests and career choice in family medicine
Most students showed little involvement in family medicine. They saw advantages and disadvantages for each of the dissimilar practices: community health centres (out-patient departments) of district hospitals, provincial hospitals and individual clinics (Table 1). In general, the participants showed equal interest in all levels of healthcare, simply more participants preferred working at the provincial hospitals because of several advantages.
| Table 1. Participants' perceptions about family practice at different sites | |
| ane. Commune health centre (CHC) | Advantages
|
| two. District hospital | Advantages
|
| 3. University medical center (equivalent to provincial hospital) | Advantages
|
| iv. Private clinics | Advantages
|
I think all levels [wellness institutions] need family doctors, because patients come to see doctors everywhere. Personally, it is about user-friendly at provincial hospitals because they concentrate many patients and there are more facilities for diagnosis and treatment. [Male student (MS), FGD-2]
Withal, they were dislocated virtually choosing family medicine as a career. Among those who were interested in the discipline, four interviewees expressed a career option for family medicine; another four participants emphasised that they would consider family unit medicine as a career option when the disadvantages were solved.
Factors influencing a career choice for family medicine
Those students who expressed their interests in a career in family medicine highly valued the relationships betwixt doctors and patients, continuing care and either a skilful work–life remainder or challenges to overcome (Tabular array 2). Students' families sometimes have a function in orienting, only not imposing on, students' career choices. The family medicine rotation had a very high impact on students, equally they could observe and participate in the clinical practice of family doctors.
| Table 2. Influencing factors to students' family unit medicine career choice | ||
| Students' characteristics | – | Gender and hometown: These were non considered as influencing factors. |
| – | Recruitment: Students who were sent for medical preparation by their provincial health departments need the health authorities' approval for their choices. | |
| – | Existing career choice: Many participants had career choices for specialties in which they would have a longer supervised preparation program and a articulate evolution pathway. | |
| – | Income: Some students estimated lower income of family doctors than specialists; some others thought income could be the same among doctors. | |
| ++ | Life balance: Family doctors might have better life rest with more patients to run across, simply non many cases requiring intensive intendance. | |
| Students' families | – | The students' families had an touch merely did not impose on students' choices. Students were influenced by family members who were healthcare workers. |
| Family medicine rotation and medical preparation programs | ++ | Family unit medicine rotation: This was very of import to students, influenced by the following factors.
|
| + | The rotations have just been taught for ii years, and their two-week elapsing was curt. | |
| + | Other reasons: At that place were many chances for postgraduate studies abroad and potential evolution in the future similar to developed countries. | |
| + | The parallel program to train upgraded fourth-yr doctors: It was not considered an influencing factor past the 6th-twelvemonth students | |
| – | Not stiff coverage of primary intendance in the curriculum; not positive attitude of the university toward chief care | |
| Value of specialty and images of family doctors | ++ | Values of specialty: Family medicine improves primary care and standing care; enhances the relationships between doctors and patients. |
| + | Images of family doctors: A few students idea family doctors should know a lot of domains/specialties, and then doctors had to be smart or hard-working; consequently, family medicine was viewed as a speciality that was too wide or too difficult past students who preferred a narrow specialty that focuses on specific diseases. In addition, a few students idea it was non a specialty that oftentimes focused on specific diseases. | |
| Sociopolitical environment and health system | –– | Health policies: They were considered to accept a large impact on students' choices.
|
| ++: positively influencing and important to students +: positively influencing but not important –: negatively influencing but not important ––: negatively influencing and important | ||
I liked to exercise in the out-patient department where I could see patients' satisfaction with a family unit medicine teacher. Some cases got more exact diagnoses considering she spent more time on history taking. I was besides interested in learning clinical cases about common problems. [FS, DI-2]
Participants saw the current sociopolitical environment mainly equally a disadvantage and one of the reasons for non choosing a career in family medicine.
I don't know much about income, only think it could be the same as that of doctors in public hospitals. The main reasons for non choosing family medicine career are that family unit medicine [master? care system] has still non been adult and not common. Patients do not know what family doctors stand for, so that limits their visits. [MS, FGD-3]
I am afraid of condign a family doctor considering information technology requires broad noesis, with footling support at the CHCs. [MS, FGD-3]
I will get bored if I work at a CHC. I will just care for unproblematic diseases and commonly refer to specialists. [MS, FGD-four]
Suggestions from the participants
For the undergraduate curriculum
The students suggested maintaining clinical educational activity methods in the family unit medicine rotation, increasing opportunities for clinical practice and keeping the module attractive with diverse case studies, multiple-pick question tests in the context of out-patient settings and family do. They liked to receive more information about family unit medicine grooming from the academy and department.
Family medicine rotation should be increased because its elapsing [two weeks] is too short for students to have many opportunities for practice. It contributes to the reason why students do not choose this specialty for their profession. [FS, FGD-ii]
The reason for non choosing family medicine every bit a career is that students do not know much about it while they are in much contact with the four specialties internal medicine, surgery, obstetrics and pediatrics. They often think about these specialties first. This specialty is quite new which makes information technology bonny for doctors who want to 'become the first' or 'make a difference'. [MS, FGD-3]
For the health regime
Healthcare policy has a large bear upon on students' choices. A good organization for family medicine practice is essential for regulations such as commencement contact, a supportive referral organisation, electronic health records, raised perceptions of patients and health professionals, and a clear pathway of professional evolution, which are all vital for students to cull a career in family medicine.
I recognise the bailiwick is very corking just I will personally non choose it as my career. When there is a modify, I will remember again. Only it might accept much time considering there are so many difficulties now. For case, the CHCs where I practised, was notwithstanding very inadequate. I feel that newly graduated general doctors working at community level should exist cautious because they are nevertheless likewise young, with too petty experience. They need a good practice site to gain more experience and support; otherwise they volition forget much knowledge learnt from university … I fright to piece of work at CHCs and district hospitals. [FS, DI-1]
The low perception of people is one of the reasons [for non following family unit medicine as a career] … Even very good family doctors cannot perform well without expert resources such as equipment, staff, and medication. Currently, most health institutions however follow 'the sometime design': there is a big need for innovation. [MS, DI-3]
Discussion
Most students in the present report did empathise and could describe well what they had learnt about family doctors, and almost the benefits of (potential) pilot family medicine clinics at each of the four different levels of intendance. Factors influencing the students' family unit medicine career choice were recognising the values of family unit medicine, particularly the person-centeredness and the long-term dr.–patient relationship; the value of the family medicine rotation and family unit medicine teachers' positive roles in information technology; and preferring a good piece of work–life balance. This finding has been found in several studies elsewhere.two,3,xi,16,25–27 In a systematic review, ii like and common factors in about countries were mentors equally role models in family medicine, and the flexibility in working conditions.28
Withal, in the present study, the number of participants who showed a career preference for family unit medicine was depression. As in many other countries, medical students prefer to get hospital-related specialists because this offers clear career development pathways, receives more than support or is less strenuous due to a smaller spectrum of clinical bug to bargain with.11,16,29–31 In add-on, the two nearly important principles of family unit medicine (continuing and comprehensive care) have not been applied commonly, fifty-fifty at pilot clinics in Vietnam. Therefore, family doctors might be recognised every bit preventive doctors or generalists. There should be conditions that are conducive to providing long-term care equally 'real family doctors', including patient allocation for family unit doctors. The Vietnamese state of affairs might reflect the earlier stages of family unit medicine development in some developed countries.11 The values of family medicine were well known past students in theory, just not articulate to them in practice. Students might be dislocated about what family doctors are well known for to attract their patients. This was also found in research in several middle- and low-income countries where the health system nevertheless had an emphasis on specialised medicine.28
Many studies on career preferences of graduating medical students that have been carried out over the past x years take been in regions where family medicine, unlike in Vietnam, has long been established (eg Europe, United states of america, Australia). Even those regions struggle to concenter sufficient numbers of graduates to family medicine, and sometimes even witness a decline.16,28,32,33 In Vietnam, it would be hard to improve primary intendance quality without support and motivation from the health system for family doctors; students wait a clearer definition of healthcare services to exist provided by family doctors, and nearly family unit doctors' career pathway development.
The family medicine rotation that has been implemented in the fifth year of medical teaching in all Vietnamese universities is only a showtime, modest step in increasing the presence of family unit medicine in undergraduate medical pedagogy. Other forms used in other countries are a preclinical family medicine elective, a four-week family medicine clerkship and a four-month family medicine rotation during the final year.2,9 Other strategies to enlarge the proportion of medical students choosing a career in family medicine are institutional reforms emphasising family medicine training and an increase in the size of the faculty.2,12,28,32
To these authors' noesis, the present study is the get-go to examine family medicine perceptions by undergraduate students in Vietnam. The strengths of the study were that it was a well-designed qualitative report, with reliable and valid data collection and analysis. A limitation of the study is that information technology was done at only 1 medical academy. Although a like perception may be expected elsewhere, the two credits of family medicine imposed on all medical faculties might not exist offered everywhere in the same manner equally at Can Tho Academy of Medicine and Chemist's shop.
The study explored the students' views to identify barriers to improving family medicine and master intendance. 2 gaps for improvement were identified. The family medicine rotation should be maintained and become more prominent in more components of the medical curriculum; and health policies to support and encourage becoming a family physician are necessary. Farther exploration of the impact of organisation approaches to family medicine is recommended.
Competing interests: None.
Provenance and peer review: Non deputed, externally peer reviewed.
Funding: None.
Correspondence to:
ttnthuy@ctump.edu.vn
guillotposinion66.blogspot.com
Source: https://www1.racgp.org.au/ajgp/2022/january-february/student-interest-in-family-medicine-in-vietnam
0 Response to "Hw Does Vietnamese Family Pick Out Healthcare Doctor in U.s"
Post a Comment